The treatment of GCT of the bone can be challenging and may include the use of medications. Sometimes tumors cannot be entirely removed using surgery or the risk of complications from surgery outweighs the possible benefit. Other times tumors recur and are not amenable to surgery. A mix of anti-inflammatories, steroids, and pain medication can be given to manage the symptoms of GCT of the bone, however, these do not treat the disease itself. In cases of either inoperable or recurrent GCT of the bone, a medical oncologist can be a vital part of a healthcare team.
Surgery can be curative for some GCT of the bone patients due to the tumor having well-defined boundary. This clear boundary allows the tumor to be completely removed during surgery. However, complete removal is not always possible. In advanced and difficult-to-access GCT of the bone, complete removal using surgery is less likely due to the size of the tumor, the possibility of extensive damage, and a lack of clear boundary. In some cases of GCT of the bone, following multiple surgeries, the tumors can recur again and again. Repeated surgery can lead to osteoarthritis and other morbidities. Therefore, pharmaceutical options are available to treat patients with inoperable and/or recurrent GCT of the bone (1).
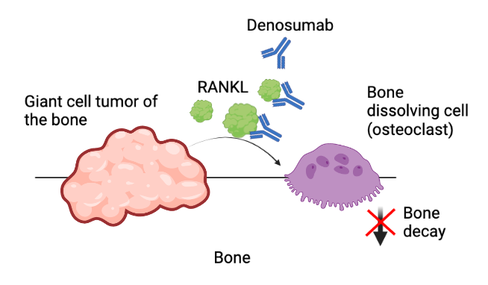
RANKL Inhibitor
Denosumab (also called Xgeva and Prolia) is a monoclonal antibody treatment that targets RANKL. A monoclonal antibody is a laboratory-designed protein that mimics the immune system and can selectively target other proteins in the body. RANKL is a protein over-produced by the GCT of the bone and leads to the bone resorption and tumor growth. Denosumab works to block the GCT of the bone from using RANKL to signal the tumor to grow and decay bone (2). To learn more about RANKL, go to Causes of GCT.
In the original clinical trial, 86% of GCT of the bone patients demonstrated tumor response (3). While denosumab does not eliminate the tumor, GCT of the bone patients also saw a reduction in their pain and improvement in their function. Other subsequent studies have found higher response rates in GCT of the bone patients, especially in "surgically unsalvageable" patients that had no disease progression following 13 months of denosumab (4,5). Patients on denosumab are also given calcium and vitamin D to reduce side effects associated with denosumab, such as reduction in calcium (hypocalcemia).
However, side effects can occur and vary in severity. However, osteonecrosis of the jaw occurs in a small subset of denosumab treated patients. It is worth noting that in approximately 5% of patients exhibited osteonecrosis of the jaw in a 5 year span in a recent study (6). Previous reports suggest the overall incidence of osteonecrosis of the jaw is 1.7% (7, 8). Additionally, long term denosumab is not well defined.
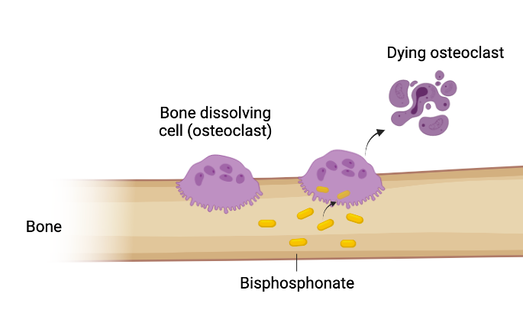
Bisphosphonates
Bisphosphonates are a group of medications that prevent and slow bone loss and strengthen bone. These medicines work by inhibiting bone dissolving cells (osteoclasts) from breaking down bone (4). The two most commonly are zoledronic acid and pamidronate. Bisphosphonates are widely used in other diseases that have bone decay, such as osteoporosis and Paget's Disease.
Bisphosphonates can be given in blood circulation through IV or can be directly injected into the tumor location, known as local administration (5, 9). Bisphosphonate can be given by itself or following surgery.
The impact of bisphosphonates on GCT of the bone is not well understood. However, it has been shown that bisphosphonates can lead to a reduction in GCT of the bone symptoms and reduce GCT of the bone growth (10, 11). While few severe side effects are seen, 1.4% of patients develop osteonecrosis of the jaw in a 5 year span according to Ehrenstein et al (6).
Consult with your healthcare provider about using bisphosphonates to treat GCT of the bone.