Ninety percent of GCT of the bone occur at the round end of long bones (called the epiphyseal of a bone). These tumors can extend into the cartilage. In rare instances where the disease impacts immature patients, such as children, the tumor is often found at the neck portion of long bones (1).
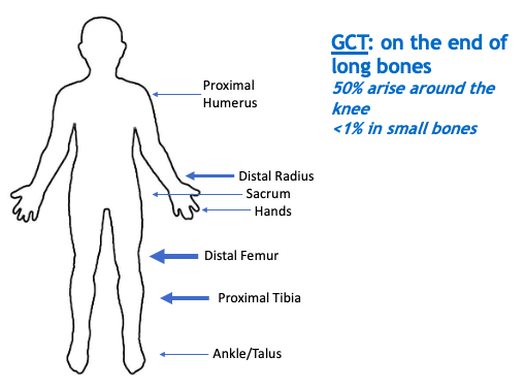
Approximately 50% of GCT of the bone are found around the knee region, with 35% being in the distal femur and 18% in the proximal tibia (2). The most common locations following the knee region are the distal radius (wrist) and the sacrum (tailbone). However, GCT of the bone can occur in the proximal femur (femoral head) and the proximal humerus (shoulder region). Other less common locations include the thoracic spine, cervical spine, skull, talus, and ulna. Small bones make up less than 1% of all GCT of the bone (3).
In 1-9% of GCT of the bone patients, GCT of the bone spreads to the lungs. In this uncommon event, the lung nodules are still considered GCT and are not cancerous. Lung metastasis is rare but more frequently seen upon recurrence rather than initial diagnosis (4). On average, lung metastasis is seen within 3 years after initial surgical resection of the primary GCT of the bone (5). Lung metastasis is influenced by many factors, including GCT grade (6). To learn more about tumor grading, go to Grades of GCT.
Additionally, location of primary GCT of the bone influences the risk of lung metastasis. For example, 13.7% of GCT patients with lung metastasis have a primary GCT of the bone site of the sacrum (7). However, the relationship between GCT location and lung metastasis is widely disputed and inconclusive.
Biannual chest x-rays or CTs are done to monitor for lung metastasis. Consult with your doctor to discuss monitoring for lung metastasis.