GCT of the bone occurs in 5% of all primary bone tumors and 20% of all benign bone tumors (1). In 90-95% of cases, a primary driver of GCT of the bone is a mutation, called the H3F3A mutation, which impacts how tightly genes within chromosomes in the GCT of the bone tumors are held (2).
In healthy cells, gene accessibility is a tightly regulated process to prevent dysfunction. Chromosomes hold genes tightly to keep normal cell function. In GCT of the bone, this regulated process is disrupted leading to chromosomes being held differently making genes more accessible for abnormal cell function. It is unknown how exactly this mutation occurs and how it directly impacts GCT of the bone growth patterns. However, in cell experiments, the addition of this mutation leads to increased giant cell growth making it a major driver for the disease (3).
In a 2018 study evaluating recurrent, metastatic, and malignant GCT of the bone cases, all cases were found to be positive for this mutation (4). This mutation is often used in pathology reports to confirm diagnosis of GCT of the bone and determine prognosis.
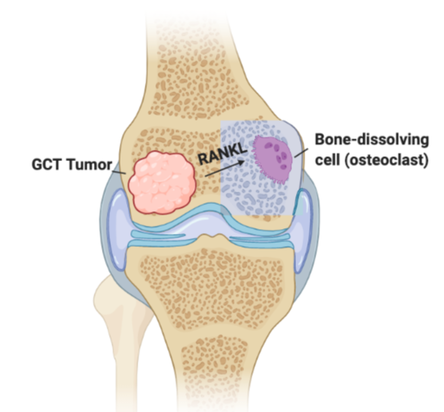
Additionally, GCT of the bone communicate with surrounding cells using the protein known as RANKL (5). This protein is also produced by bone-dissolving cells, which GCT of the bone have common features with. GCT of the bone signals to bone-dissolving precursor cells to dissolve bone while the tumor continues to grow through the over-production of RANKL. This enhanced signaling of RANKL leads to bone decay and overall destruction of the limb. Therefore, the major medication treatment for GCT of the bone blocks the signaling of RANKL.